


Framing the shift: why models matter
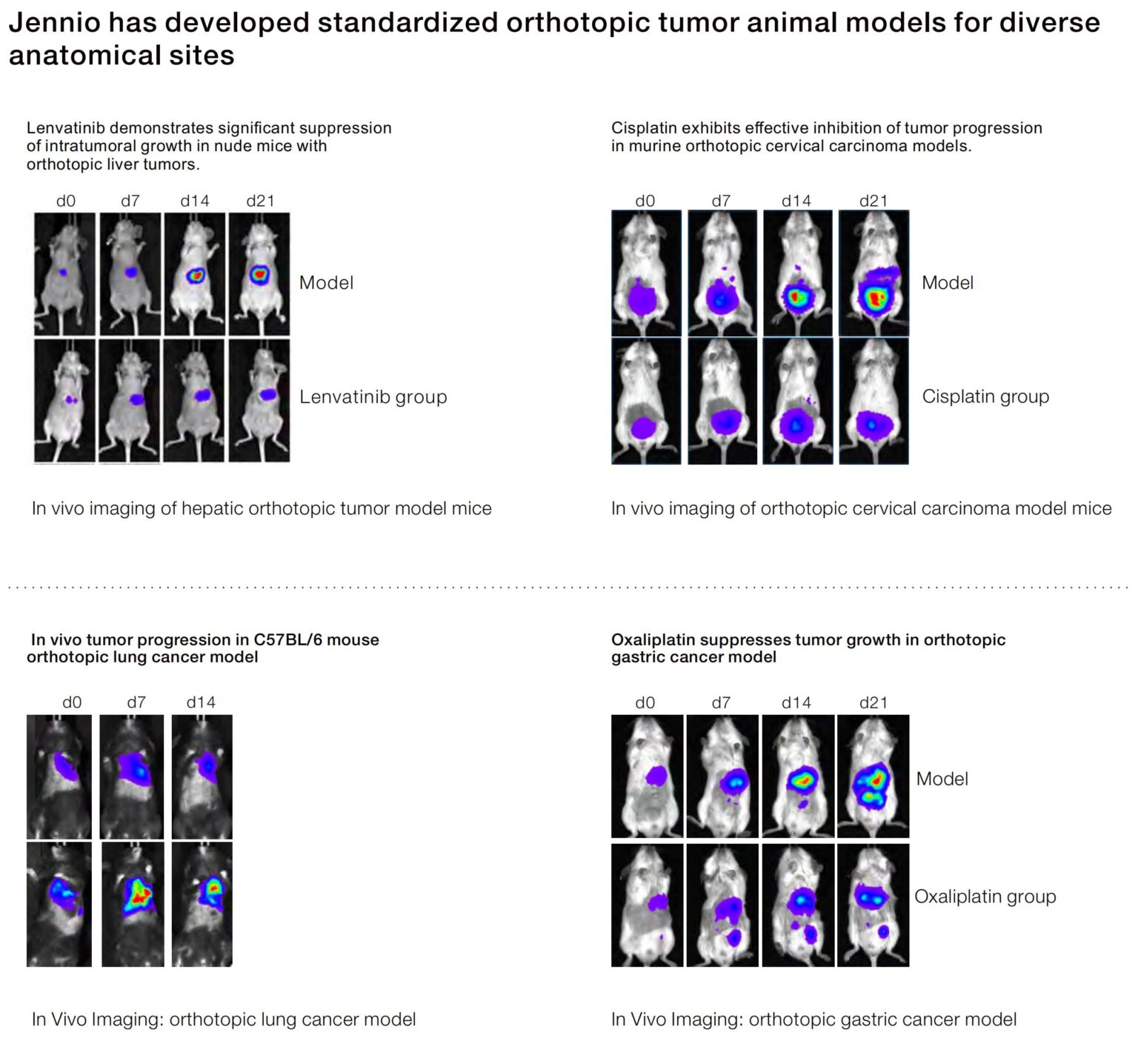
The story of immuno-oncology is inseparable from the models that test its hypotheses. Early reliance on simple subcutaneous xenografts gave way to organ-aware systems as researchers recognized that anatomical context and immune interactions dictate therapeutic outcomes. This turning point pushed investigators toward models such as the orthotopic tumor model, which reintroduces the tumor into its native site and thereby preserves key facets of the tumor microenvironment and metastatic routes.
Milestones along the arc
Two parallel forces drove model evolution: clinical demand for translational fidelity and technical progress in engraftment and mouse humanization. The field’s broader validation came into sharp relief after the 2018 Nobel Prize in Physiology or Medicine recognized discoveries that harnessed immune checkpoints—an event that crystallized the need for preclinical systems that reflect immune-tumor dynamics. Patient-derived xenograft (PDX) models and organ-specific implants began to replace generic implants because they better preserve heterogeneity, stromal interactions, and pharmacodynamic responses.
Core differences: what orthotopic and PDX models capture
Orthotopic placement and PDX approaches capture three critical features that subcutaneous models miss: native extracellular matrix composition, realistic vascularization, and pre-metastatic niche formation. These elements influence immune cell trafficking and checkpoint blockade efficacy. Terms to keep in view include xenograft, tumor microenvironment, and engraftment rate—each tied to measurable experimental outcomes such as take rate, immune infiltration indices, and response durability.
Alternatives and when to choose them
Not every question demands an orthotopic or PDX study. Syngeneic models retain an intact mouse immune system and excel when interrogating host-immune mechanisms or early-stage discovery. Humanized mice are preferable when human immune components are essential. In vitro organoids and 3D co-cultures provide rapid mechanistic insight and high-throughput screening capacity. Each alternative trades translational fidelity for throughput or cost; matching model features to a precise endpoint is essential.
Common mistakes and how to avoid them
Investigators often err by prioritizing convenience over context: high tumor take rates in subcutaneous sites do not guarantee predictive value for immune-targeting agents. Another frequent error is insufficient reporting of engraftment conditions and passage history—details that alter tumor biology across experiments. Standardize implantation coordinates, report donor characteristics for PDX tissues, and quantify immune infiltration with objective metrics such as CD8+/FoxP3 ratios—these steps reduce ambiguity and increase reproducibility. —A small investment in metadata saves months of follow-up work.
Practical metrics for model selection
Choosing the right model requires clear evaluation metrics. Consider the following when planning studies: translational relevance (histological fidelity to the originating tumor), immune fidelity (presence and function of human immune components or validated murine correlates), and technical reproducibility (take rate, latency, and inter-animal variance). Track pharmacodynamic markers aligned with the therapeutic mechanism—PD-L1 modulation, cytokine signatures, or tumor-infiltrating lymphocyte density—to link preclinical outcomes to clinical hypotheses.
How in situ approaches integrate with broader workflows
In situ model system patient tumor strategies combine organ-specific architecture with patient-derived material to yield a high-fidelity bridge to the clinic. Integrating these models into early translational workflows clarifies dosing windows, safety margins, and combination opportunities with checkpoint blockade or cellular therapies. When paired with robust biomarker panels, they sharpen go/no-go decisions and reduce costly late-stage failures.
Advisory: three golden rules for selecting tumor models
1) Align the model to the decision point: prioritize throughput for target ID, fidelity for translational testing. 2) Insist on immune-context metrics: measure immune cell composition, cytokine response, and functional assays that match your therapeutic class. 3) Demand repeatability: require documented take rates, passage histories, and standardized implantation protocols before scaling studies.
These rules culminate in one practical conclusion: choose models that answer the question you will face in the clinic — and document them rigorously. Jennio Biotech provides organ-aware, patient-derived solutions that make those choices actionable—trusted tools that translate experimental rigor into clinical clarity. —Final thought: fidelity matters.